The Addiction Conundrum
By Monica E. Oss, Chief Executive Officer, OPEN MINDS
May 28, 2025
About 9.7% of U.S. adults with an addiction disorder in 2022 were hospitalized in the prior year—compared to the 8.4% hospitalization rate among adults in the general population, according to recent research published in Prevalence Of Hospitalizations Among A National Sample Of U.S. Adults With Substance Use Disorders. It doesn’t sound like a lot. But there were 34 million hospital admissions in the U.S. in 2023. And that 1.3% difference is about 442,000 admissions.
In total, 60 million adults in 2022 had an addictive disorder, and 5.8 million of them were hospitalized. And the study authors observe that the identified hospitalization rate is likely understated because it does not account for readmissions.
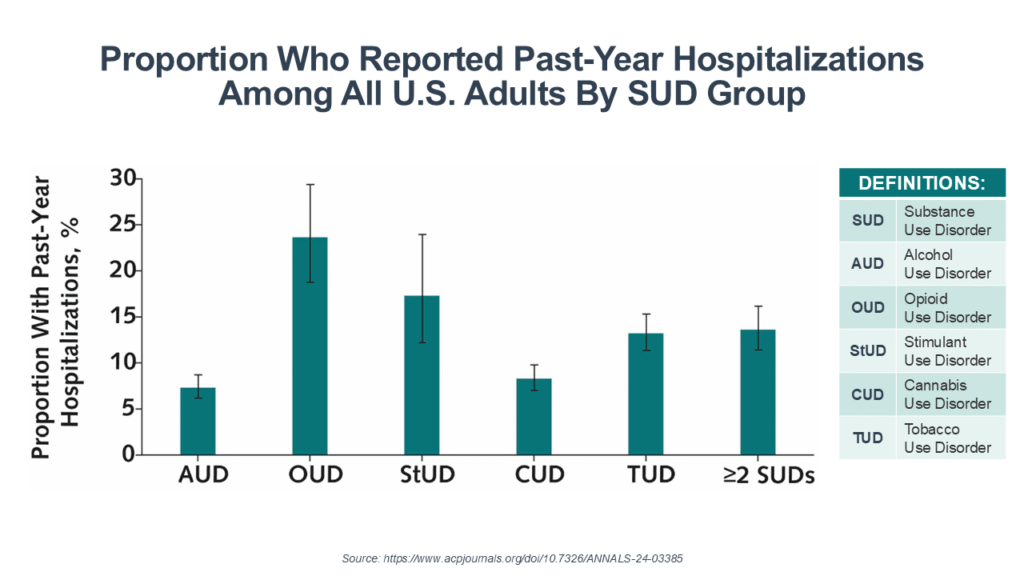
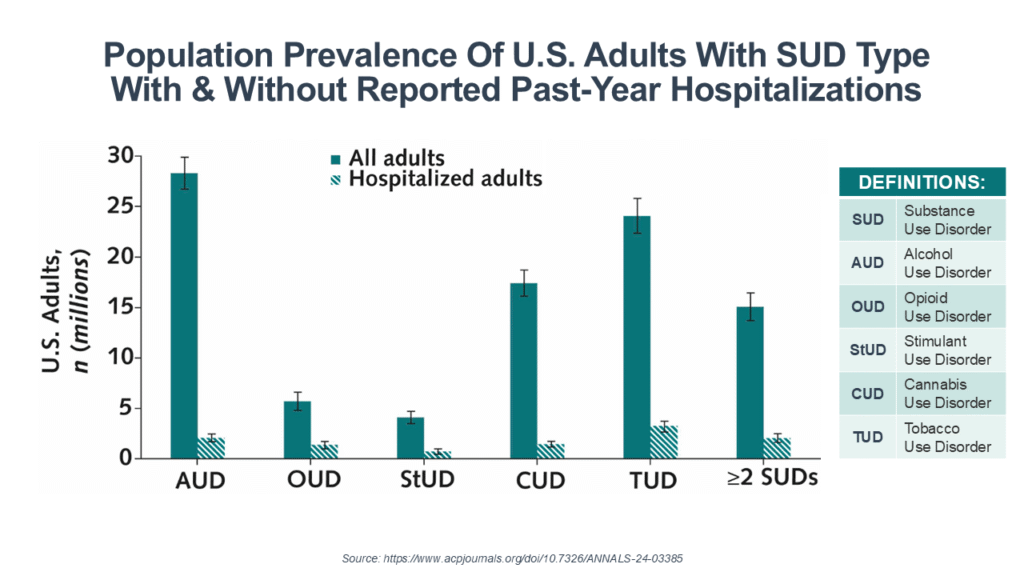
The hospitalization rate for those with an addictive disorder varied by substance from the low of 7.3% among those with alcohol use disorder (AUD) to the high of 23.6% among those with opioid use disorder (OUD). But the population prevalence makes them both a big issue—with 28.3 million people with AUD and 5.7 million with OUD.
Compared with non-hospitalized adults with a substance use disorder (SUD), those with past-year hospitalizations were more likely to be older and were more likely to have 2 or more comorbid medical conditions. And among those with alcohol, cannabis, and tobacco use disorders, hospitalized adults were also more likely to have a serious mental illness.
For executives of health and human service organizations, the excess use of hospitalizations due to addictions is both a challenge and an opportunity. The challenge—any performance-based contract that has admissions or readmissions as a measure of performance is going to be negatively affected by consumers with untreated addictions. Readmission rates and emergency room utilization were ranked second and third as the most common factors in value-based reimbursement arrangements with specialty provider organizations.
Payer and health plan executives are aware of these excess costs and are looking for solutions. David Lederman, Senior Product Manager at Elevance Health, spoke at The 2023 OPEN MINDS Strategy & Innovation Institute about their data showing that total cost of care doubles for members with any behavioral health condition. Those costs triple for those with OUD. And IV drug users actually had 77% higher total costs of care.
The opportunity for provider organization strategy is developing solutions to address this issue—focusing on programmatic approaches to manage the total costs of care of consumers with addictive disorders.
I asked my colleagues, OPEN MINDS Executive Vice President Kim Bond and Senior Associate Deanne Cornette, for their perspectives on how provider organization executives can develop new revenue streams addressing this issue. Ms. Bond spoke to the shifting characteristics of substance abuse, “As new adulterants in street drugs drive up physical health complications, behavioral health provider organizations need to adjust their clinical approaches.”
She pointed to organizations that are already pursuing new program and licensure models so they can bill for physical health care alongside substance use treatment. “It’s a necessary move, because many clients are recovering from drug-related conditions that current SUD billing rules don’t cover. Without integrated services, providers face a tough choice—absorb the cost of care or discharge clients to under-resourced facilities, including homeless shelters.” Her advice was direct: “Start moving now to incorporate primary care into your service array,” regardless of whether your organization primarily focuses on substance use, mental health, or intellectual and developmental disabilities.
Ms. Cornette focused on the strategic and financial dimensions of the crisis. She noted, “The opioid crisis has entered a new phase… For community-based provider executives, it’s not just a clinical challenge—it’s a business imperative. Preventable hospitalizations and crisis events are costly, and under value-based contracts, they ‘eat directly into margins’.”
Her advice? “Sharpen your data lens.” She urged managers to develop real-time data capabilities—by zip code, age group, and race—to support earlier interventions and better resource allocation—and new treatment approaches. “The old model of requiring someone to seek treatment on your terms does not work… harm reduction strategies, same-day medication starts, and community-based outreach must become the new standard.”
Ms. Cornette also underscored the importance of having a well-defined financial strategy. “Accessing Medicaid waivers or opioid settlement dollars takes a clear plan, strong data, and evidence that your model can reduce emergency care use… Done right, these strategies don’t just reduce financial risk—they open up new funding streams and strengthen long-term sustainability.”
Want to Read more?
To view this content, please sign up or log in to your account.
Create an account in seconds or log in if you’re already a member.


