The Opioid Hat Trick
By Monica E. Oss, Chief Executive Officer, OPEN MINDS
July 29, 2025
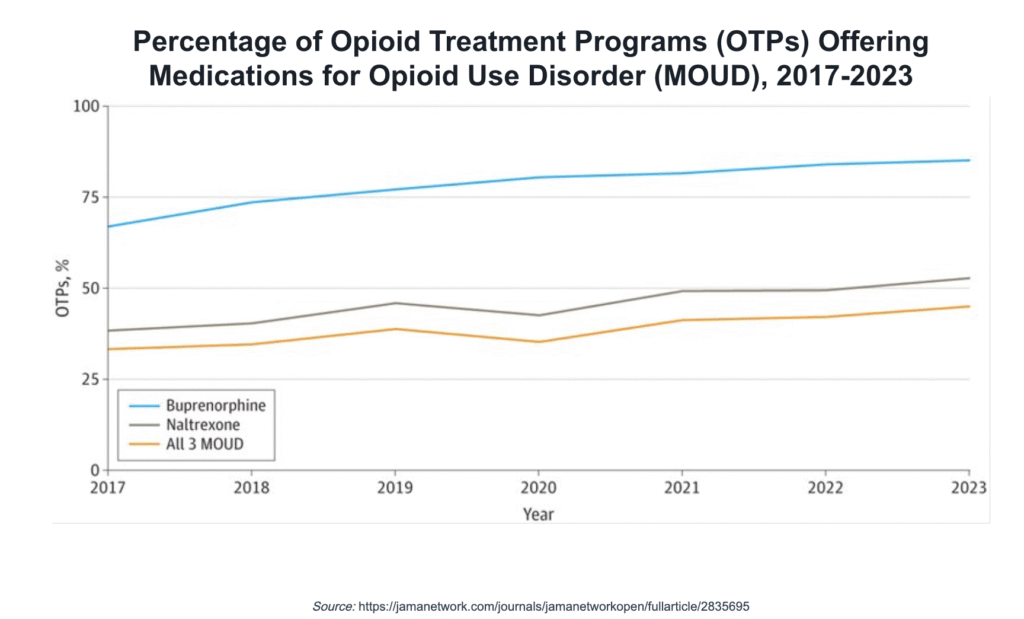
The availability of medications for opioid use disorder (MOUD) has increased—but still doesn’t reflect the availability of medications for other health conditions. About 45% of opioid treatment programs (OTPs) offer all three approved medications for opioid use disorder (MOUD)—methadone, buprenorphine, and naltrexone – according to a recent report, Availability Of Medications For Opioid Use Disorder In Opioid Treatment Programs. The percentage of OTPs offering the full range of MOUD increased from 33% in 2017, but uptake of buprenorphine and naltrexone has been uneven.
All the OTPs surveyed offer methadone. The percentage of OTPs offering buprenorphine increased from 67.0% in 2017 to 85.1% in 2023. The percentage of OTPs offering naltrexone increased from 38.2% in 2017 to 52.7% in 2023. OTPs can be structured as non-profit or for-profit, private or public, standalone or part of a larger program that provides multiple levels of services. They must be licensed and registered with the federal Drug Enforcement Administration (DEA). OTPs are typically open 6 or 7 days a week.
The type of MOUD offered varied significantly by the ownership structure of the OTP. Government-operated OTPs were more likely to be comprehensive medication OTPs (those offering all three approved MOUD medications). These government-owned OTPs represented 6.7% of all programs—7.2% of those offering buprenorphine, 10.6% of those offering naltrexone, and 11.3% of those offering all three MOUD.
Private, for-profit OTPs represented 57.6% of programs—59.4% of those offering buprenorphine, 46.5% of those offering naltrexone, and 46.4% of those offering all three MOUD. Private, non-profit OTPs represented 24.2% of programs—23.7% of those offering buprenorphine, 33.9% of those offering naltrexone, and 33.2% of those offering all three MOUD.
At the consumer level, access to MAT treatment remains low across multiple populations. Among the 1.5 million Medicaid enrollees with OUD, only two-thirds received treatment in 2021. And only 22.3% of the 2.5 million adults in the U.S. with past-year OUD received MAT.
The results are obvious. Provisional data from the CDC’s National Center for Health Statistics shows an estimated 80,391 drug overdose deaths in the U.S during 2024—a decrease of 26.9% from the 110,037 deaths estimated in 2023. Still an alarmingly high number.
This situation exists despite the fact that the use of MAT for OUD treatment, which has been referred to as the “gold standard” for treatment. But that endorsement hasn’t been enough to drive the adoption of MAT, even though health and human service (HHS) executives—at the policy and practice level—are trying to drive the use of medications in treatment. But the barriers are many.
On the consumer side, logistical barriers are a significant roadblock to accessing MAT. 69% of consumers identified transportation challenges and limited access to cell phones, particularly for telehealth services, as key obstacles. And nearly 40% of consumers pointed to lack of insurance as a critical factor impeding access to care. Almost a third of consumers reported they were mistrustful of the health system as a result of prior poor treatment. As a result, 13% of consumers were reported to have refused MAT as treatment.
On the provider side, 46% of clinicians had difficulty engaging consumers for treatment, while a third reported that stigma is an issue—citing apprehension about the clinical complexity of cases and negative stereotypes about individuals with OUD. A reported 14% of clinicians reported not viewing MAT as a best practice for treating OUD.
For more on what this means for provider organization executives, I reached out to my colleague and OPEN MINDS Senior Associate, Sharon Hicks.”Health care provider organizations should be doing screenings for substance use when indicated, whether they offer treatment programs or not. There are evidence-based screening instruments for alcohol and drugs, which should be standardized into workflows. Ask questions—administer the screeners and ask if anyone has ever spoken with them about their use of drugs or alcohol,” Ms. Hicks said.
But she noted that screening isn’t enough without follow through. “Any consumer who has an alcohol use disorder or OUD should be referred for an evaluation for MAT. The science is unequivocal that MAT is effective and that it is the best, first line of care. What leadership teams can do is create a process that ensures that all people in need of it receive information about MAT. Standardized patient information should be part of the protocol, whether you offer the service or you need to refer it.”
To get these protocols in place and make them happen, Ms. Hicks added, “Clinician training and education to standardize screening, provide patient information, and direct people into your services or to your partners in the community is the first and most necessary step. Make sure everyone is aligned, trained, and prepared. And to ensure that MAT is fully integrated across the continuum of care, managers must also confront some of the entrenched barriers that inhibit access and scale. These include persistent stigma, fragmented funding mechanisms, and restrictive insurance policies.”
“Screen, inform, and treat or refer, Ms. Hicks said. “It’s as much a process improvement question and a workflow question as it is a clinical question.”
Want to Read more?
To view this content, please sign up or log in to your account.
Create an account in seconds or log in if you’re already a member.


