The Stigma Gap
By Monica E. Oss, Chief Executive Officer, OPEN MINDS
July 14, 2025
Pulling together some recent data for a market analysis, I was surprised at the different trajectory for treatment between mental illnesses and addictions. In the U.S. in 2022, 23.1% of the population had a mental illness of some type, and 50.6% of those people got treatment for that mental illness. But, of the 11.8% of the population with a substance use disorder (SUD), only 6.5% got treatment in 2024.
The differences in the statistics certainly raise questions. Are these numbers due to the availability of the clinical workforce? Differences in reimbursement for treatment? Faulty data? My initial thought is that while the pandemic did a lot to destigmatize mental health issues—and pushed up both self-identification and demand—that does not appear to be the case with addictions.
The research supports this contention. People were found to have developed a more nuanced understanding of mental health both in themselves and others during the pandemic. This includes both increased awareness of their own mental health status, as well as decreased unfavorable perceptions of others with mental illness and/or who received mental health care. This change was attributed to experiencing poor mental health and discussions of the importance of mental health, whether in the media or personal conversations.
With that in mind, the recent OPEN MINDS Executive Roundtable, Addressing Addiction Stigma Among Clinicians: The Shatterproof ‘A Provider’s Pathway’ Curriculum, provided a lot to think about. Courtney McKeon, Senior Vice President, and Robert DeForde, Program Manager, Shatterproof National Stigma Initiative, discussed their Shatterproof Addiction Stigma Index (SASI) and its implications for the field and the health care system.
Connecticut-based Shatterproof is a $23.5 million non-profit advocacy organization focused on improving addiction treatment and access through consumer outreach, education to address stigma, and advocacy for policy changes. Shatterproof has also created partnerships with leading experts in the field to document and publish its National Principles of Care, as well as launched the Treatment Atlas (Atlas), a public-facing portal containing provider-level data that helps consumers find and assess SUD treatment programs.
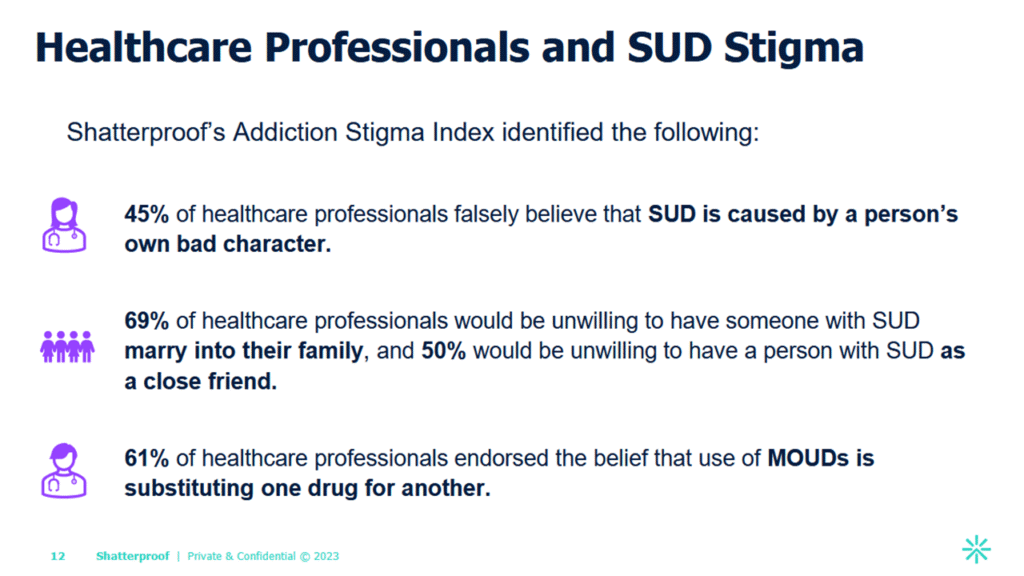
In 2021, Shatterproof launched its Shatterproof Addiction Stigma Index (SASI) in partnership with Indiana University and Ipsos. It is a tool designed to assess levels of stigma using 50 validated stigma measures and four stigma indices that measure public, structural, self, and Medications for Opioid Use Disorder (MOUD) stigma.
The findings of national surveys using the tool are that 67% of health care professionals do not believe SUD is a chronic medical condition, 45% attribute SUD to “bad behavior,” and 61% view medication-assisted treatment (MAT) as simply substituting one drug for another. In addition, 69% of health care professionals would be unwilling to have someone with SUD marry into their family, and 50% would be unwilling to have a person with SUD as a close friend.
Ms. McKeon noted that this stigma among clinical professionals has many effects. Most importantly, there is a general reluctance to treat people with addictions, a lack of medication-assisted therapies offered to consumers, and inadequate pain management. In addition, she noted that among people who know they need SUD treatment but do not receive it, 10.4% cite the fear of attracting negative attitudes from their communities as a reason to not seek treatment.
The question for executive teams is what to do to change this stigma toward consumers with addictions. The speakers advised three approaches: measure existing staff stigma, adopt stigma reduction training, and build a patient-centered organizational culture.
Executives must first identify how prevalent stigma is among their clinical staff by measuring internal attitudes using validated tools. This initial step will identify training needs and allow organizations to track stigma change over time.
The second, and biggest step, is for executives to integrate stigma reduction training into clinical onboarding, continuing education, and leadership development. This approach should include mentorship for new clinicians and provide ongoing resources like stigma-reduction workshops and peer learning. The key is to understand that this training should be focused on changing behavior, not just giving clinicians new knowledge. The critical and practical skill that training should impart is the ability to interact with and support colleagues and patients experiencing SUD challenges.
And finally, executives need to drive a consumer-centered organizational culture. This overall approach to improving consumer experience, consumer satisfaction, and consumer outcomes will lead to reductions in stigma as part of performance improvement initiatives.
“This should be a part of the culture of an institution,” said Mr. DeForde. “We hear all the time, when we look at the missions and value statements of institutions, about how patient-centered care is so important. But that’s not just patient-centered care when someone has a flu or they show up in the ER with a broken arm. It’s also about patient-centered care and compassionate care when they show up in one of the most difficult points in their life.”
Want to Read more?
To view this content, please sign up or log in to your account.
Create an account in seconds or log in if you’re already a member.


